Colorectal Cancer
Introduction

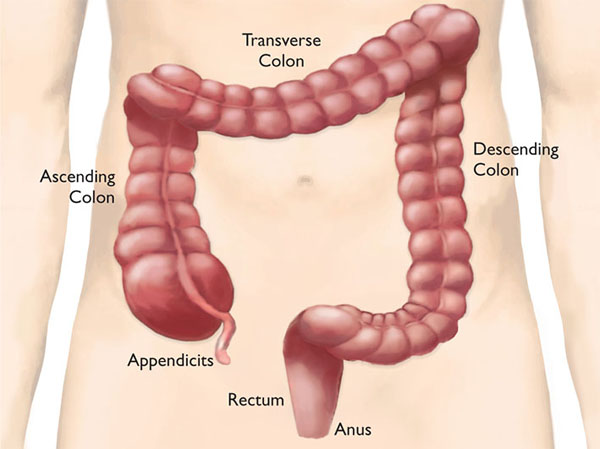
Colorectal cancer is cancer of the colon and rectum (or the large intestine), which is the last part of the gastrointestinal tract. When food enters the colon, water is absorbed and the food residue is converted into waste (faeces) by bacteria. The rectum is the terminal part of the colon that stores faeces before it is expelled through the anus. Polyps may form on the inner wall of the colon and rectum. These are benign lumps which are fairly common in people above the age of 50. However, certain types of polyps may develop into cancer and should be removed if they are detected.
Certain characteristics of a polyp may indicate malignancy:
- Polyps greater than 1 cm in diameter
- Sessile polyps (i.e. polyps without a stalk)
- Multiple polyps
In the early stages of colorectal cancer, the cancer cells are confined to the colon. If undetected, the cancer will develop and project into the lumen of the colon. It will also invade through the colon wall and spread by:
- Invading neighbouring intestines and organs
- Entering the lymphatic system and travelling into neighbouring lymph glands (mesenteric lymph nodes)
- Entering the blood stream and travelling to the liver where secondary malignant deposits may form
Risk Factors
Age
Men and women aged 50 years and above have an increased risk of colorectal cancer
Ethnicity
Among the races in Singapore, the Chinese have a higher risk of colorectal cancer.
Personal History
Individuals who have been detected with colorectal polyps or diagnosed with colorectal cancer in the past may be at a higher risk of experiencing a recurrence and are advised to seek regular screening.
Family History
Some individuals inherit a rare disease called familial polyposis in which many colorectal polyps develop at a young age. For these individuals, the risk of developing colorectal cancer is very high (80 to 100%). Such individuals should consider having the colon removed before the age of 40. Individuals who have relatives with polyps or colorectal cancer are also at a higher risk of colorectal cancer although this risk is lower compared to one with familial polyposis.
Ulcerative Colitis
This is a disease affecting the bowels which, in the long term, leads to inflammation and cancerous changes. People with with this condition have a significant risk of colorectal cancer.
Drugs
Current users of HRT (hormone replacement therapy) are at a lower risk of colorectal cancer, although this protection disappears within 5 years of stopping HRT. Aspirin and NSAID (a strong painkiller drug) are known to reduce the risk of colorectal cancer. However, it is premature to recommend the routine use of these drugs for this purpose.
Sedentary lifestyle and obesity
These interrelated factors increase the risk of colorectal cancer. However, physical activity improves the movement of faeces in the colon and can reduce risk.
Dietary Habits
Research has identified certain factors which can affect the risk of colorectal cancer.
Dietary factors that may increase colorectal cancer risk are processed and red meat, meat cooked at high temperatures, and alcohol.
Dietary factors that may reduce colorectal cancer risk are fruits and vegetables and dietary fibres .
Despite knowledge of these risk factors, the exact cause of colorectal cancer is unknown. It is estimated that 50 per cent of colorectal cancer patients have no known risk factors.
Signs & Symptoms
Although colorectal cancer often has no symptoms at an early stage, warning signs that you should look out for include:
Blood in your stools
Change in bowel habits
Abdominal pain or discomfort
Anaemia (a low red blood cell count)
Presence of a lump in the abdomen
Early Detection and Screening
Regular screening can detect polyps or colorectal cancer early. Several different tests can be used. Each can be used alone. The Faecal Immunochemical Test (FIT), a recommended test, is a quick and convenient screening test to detect early stages of colorectal cancer. Usually, FIT is done first and if the results are positive, it will be followed by one of the other tests.
Faecal Immunochemical Test (FIT)
Colorectal polyps and cancers can bleed into the colon. The amount of bleeding may be small and invisible to the naked eye. FIT is a preliminary test that detects the presence of small amounts of blood in faeces. This simple test is available in a kit and can be carried out in the comfort of your own home.
SCS has ceased FIT kit distribution. Please collect your FIT kits through your Healthier SG healthcare provider, subject to screening eligibility. Kindly note that doctor consultation and screening test fees may apply.
Colonoscopy
This test involves the examination of the colon and rectum using a flexible fibre-optic instrument introduced through the anus under sedation. In addition to its diagnostic use, a colonoscopy can be used for treatment, such as removing polyps, biopsying cancerous lumps, and staunching bleeding spots. Colonoscopy is a safe procedure with a low incidence of complications and is recommended to be done once every 10 years.
Diagnosis
Besides the list of signs and symptoms, a doctor may conduct further procedures to confirm a diagnosis and determine whether the patient is at high or low risk.
Colonoscopy
In addition to diagnosing colorectal cancer it can also be used to check the entire length of the colorectum for other traces of cancer or the presence of polyps. At the same time, cancer that has been detected can be biopsied or polyps removed.
CT Scan
This detailed computerised X-ray scan is especially useful for determining the actual extent and location of a cancerous tumour, the invasion of adjacent organs or bowels, and the presence of liver metastases. A cheaper alternative to a CT scan is an ultrasound scan, which is accurate for diagnosing liver metastases.
Tumour Makers
The tumour marker for colorectal cancer is carcino-embryonic antigen (CEA). Patients with colorectal cancer may have a high level of CEA. These cancer-specific substances are found in the blood and are useful in monitoring patients for the recurrence of cancer after surgery.
Biopsy
A diagnosis of cancer is based on a biopsy of polyps or tumours. A tissue sample of the tumour is removed and sent for laboratory analysis.
Treatment
Surgery is the primary form of treatment for earlier-stage colorectal cancer. The aim of surgery is the complete removal of the cancerous sections of the colon and/or rectum, as well as its surrounding tissue and mesenteric lymph nodes. After removal, the two unconnected ends of the bowel are joined together (anastomosis).
Depending on the type and extent of the surgery performed, a colostomy may be sometimes necessary. A colostomy involves creating a new opening (stoma) in the abdomen which will be connected to one end of the colon to enable the discharge of faeces. The patient will have to wear a colostomy bag to collect faeces and learn how to clean and care for the stoma and surrounding skin. This process may be temporary or permanent.
As a temporary measure, a colostomy diverts the faeces and allows the anastomosis to heal. Once healed, the colostomy is closed in a second operation.
For rectal cancers situated close to the anus, treatment may involve the complete removal of the anus as well, which may necessitate a permanent colostomy in the lower right abdomen.
In order to avoid a permanent colostomy, new surgical techniques have been developed to retain the anus. The first method entails performing intestinal anastomosis as close to the anus as possible using mechanical staples rather than hand sewn stitches (sphincter saving surgery). The second method entails creating a new anus using muscles from the thigh (neo-sphincter surgery).
Surgery in special situations:
1. Liver metastasis
In a healthy patient with few isolated liver metastases, their removal can be performed at the same time as excision of the cancerous areas. However, this is often not viable. As such, patients with colorectal cancer and liver metastases are commonly treated with chemotherapy.
2. Large inoperable tumour
Should a tumour in the colon or rectum grow too large, intestinal bypass surgery is required to relieve bowel obstruction.
3. Colorectal cancer causing intestinal obstruction or perforations
In this acute situation, the patient will require emergency surgery to relieve the obstruction or to stem the leakage of faeces. When the patient has sufficiently recovered, a second or third operation may be necessary to remove the tumour and reconnect the intestines.
Laproscopic Colon Surgery (also known as Keyhole Surgery)
Colorectal cancer has been treated using this minimally invasive technique. Its advantage is less pain and quicker post-operative recovery. However, it is technically difficult, time consuming, and expensive to carry out. Laparoscopic surgery might not be the best approach for everyone. Please discuss with your doctor if you are considering this type of surgery.
Chemotherapy
Chemotherapy is the administration of toxic drugs to kill cancer cells which may be found at the site of the cancer or elsewhere in the body after surgery. It is indicated for patients with advanced colorectal cancer at stages II, III or IV after surgery and improves survival rates. Chemotherapy usually involves the weekly injection of a cytotoxic drug called 5FU (5 Flurouracil) alone or in combination with other drugs for up to a year.
Because of its toxicity, chemotherapy causes significant side effects. The immediate side effects include nausea, vomiting, diarrhoea, susceptibility to infection, low white cell counts, and hair loss. The long-term side effects include premature menopause and risk of a second cancer.
Radiotherapy
Radiotherapy is the administration of powerful radioactive rays to treat cancer. Its role in the treatment of colorectal cancer is secondary to surgical excision and is used in the following situations:
- After the surgical removal of a colorectal cancer which has invaded the adjacent organs and/or nearby lymph nodes to destroy residual cancer cells within the site of the cancer.
- During the pre-operation phase, it is used on a locally advanced rectal cancer to shrink it to a size where it can be surgically removed.
Radiotherapy is administered in daily sessions, 5 days per week over 4 to 6 weeks. Side effects are usually tolerable and temporary and range from abdominal cramps and pain, constipation or diarrhoea, cystitis, excoriation of perianal skin, and generalised tiredness.
Pre-Operation Preparation
Colorectal cancer surgery is a major operation. Careful preparation before the operation is of the utmost importance.
- Individuals above the age of 70 or those with chronic diseases such as diabetes, hypertension, and stroke as well as liver, heart, lung, or kidney problems) are at a higher risk from undergoing surgery and general anaesthesia. Their fitness will be carefully assessed for surgery and general anaesthesia.
Preparations:
|
Patients who have: |
Pre-operation Preparations: |
|
Poor lung function or smoke |
Smoking cessation Breathing exercises |
|
Ischaemic heart disease and are on anti-platelet therapy |
Cardiac assessments Stop taking anti-platelet drugs Albumin transfusion |
|
Hypertension or diabetes mellitus |
Careful management of blood pressure or blood sugar levels before the operation |
- The patient’s colon is cleansed of faeces before the operation to prevent contamination at the time of surgery. The patient is admitted before the operation and given purgatives. Patients are only permitted a liquid low fibre diet for a few days before the operation.
- As colorectal surgery involves coming into contact with faeces, a strong antibiotic is administered before the operation.
Post-Operation Period
This crucial period lasts about one week long as the patient recovers from the operation. The patient may develop a complication such as a lung infection or leakage from the anastomosis. He/she may be put on an intravenous drip to supply fluids. After recovering intestinal function and the ability to eat and drink, the intravenous drip is stopped. Medication needed during this period includes antibiotics and strong painkillers.